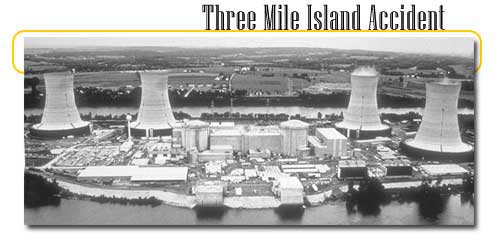
Three Mile Island is the location of a U.S. nuclear power plant that, on March 28, 1979, suffered a partial core meltdown. The Three Mile Island Nuclear Generating Station sits on the island in the Susquehanna River in Dauphin County, Pennsylvania, near Harrisburg, of area 3.29 km² (814 acres).

The accident unfolded over the course of five tense days, as a number of agencies at the federal, state, and local level attempted to diagnose the problem (the full details of the accident were not discovered until much later), and decide whether or not the on-going accident required a full evacuation of the population. In the end, the reactor was brought under control. No identifiable injuries due to radiation occurred (a government report concluded that "the projected number of excess fatal cancers due to the accident ... is approximately one."), but the accident had serious economic and public relations consequences, and the cleanup process was slow and costly. It also furthered a minor decline in the public popularity of nuclear power, exemplifying for many the worst fears of nuclear technology, and until the Chernobyl accident seven years later was considered the world's worst civilian nuclear accident.

The accident had a number of primary causes, related both to technical malfunction and human error. The accident in the TMI-2 reactor (the plant had two reactors; TMI-1 was down for refueling at the time) began when the plant's main feedwater pumps in the secondary non-nuclear cooling system failed. This failure was due to either a failure in the condensate system and caused a reduction in feedwater flow which prevented the steam generators from removing heat. First the turbine, then the nuclear reactor automatically shut down. Immediately, the pressure in the primary system (the nuclear portion of the plant) began to increase. In order to prevent that pressure from becoming excessive, the pressurizer relief valve opened. The valve should have re-closed when the pressure decreased by a small amount, but it did not. The only signals available to the operators showed the valve as being closed, but in fact only the signal to close the valve was sent. The "positive feedback" lamp in the control room indicating the true position of the valve (a Pressure Operated Relief Valve, or PORV) was eliminated in original construction to save time and has been backfitted to all other similar plants. As a result of this error in the design this stuck-open valve caused the pressure to continue to decrease in the system.
Meanwhile, another problem appeared elsewhere in the plant to the emergency feedwater system (the backup to the main feedwater). It was tested 42 hours prior to the accident. As part of the test, a valve is closed and then reopened at the end of the test. But this time, through either an administrative error, or human error, the valve was not reopened. This prevented the emergency feedwater system from functioning during the accident. The valve was discovered closed about eight minutes into the accident. Once it was reopened, the emergency feedwater system began to work correctly, allowing cooling water to flow into the steam generators.
As the system pressure in the primary system continued to decrease, voids (areas where there is no water present) began to form in portions of the system other than the pressurizer. Because of these voids, the water in the system was redistributed and the pressurizer still had water available. The turbulence as this water blew out the stuck-open valve caused the level indicator to think the pressurizer was full. Thus the level indicator, which tells the operator the amount of coolant capable of heat removal, incorrectly indicated the system was full of water. Therefore, the operator stopped adding water — by turning off the Emergency Core Cooling pumps, which had automatically come on.
After almost eighty minutes of slow temperature rise the primary loop pumps began to shudder as steam rather than water began to pass through them. The pumps were shut down, and it was believed that natural circulation would continue the water movement. Steam in the system locked the primary loop, and as the water stopped circulating it was converted to steam in increasing amounts. After around 130 minutes since the first malfunction, the top of the reactor core was exposed and the heat and steam drove a reaction involving hydrogen and radioactive gases with the zirconium nuclear control rod cladding. The quench tank (collecting the discharge from the PORV) overfilled, its relief diaphragm ruptured, and radioactive coolant began to leak out into the general containment building. A new arrival noticed that the temperature in the holding tanks was excessive and used a backup valve to shut off the coolant venting, but around 250,000 US gallons (950 m³) of coolant had already leaked from the primary loop. It was not until 165 minutes after the start of the problem that radiation alarms activated as contaminated water reached detectors - by that time the radiation levels in the primary coolant water were around 300 times expected levels, and the plant was seriously contaminated.
It was still not clear to the control room that the primary loop water levels were low and that over half of the core was exposed (a LOCA). Around seven hours into the emergency, new water was pumped into the primary loop. After almost sixteen hours the primary loop pumps were turned back on and the core temperature began to fall. A large part of the core had melted and the system was still dangerously radioactive. Over the next week the steam and hydrogen were removed from the reactor using a recombiner and, more controversially, by venting straight to the atmosphere. It is estimated that a maximum of 13 million curies of radioactive noble gases were released by the event, though very little of the hazardous iodine-131 was released.
"Despite melting of about one-third of the fuel, the reactor vessel itself maintained its integrity and contained the damaged fuel." According to sources, "The average radiation dose to people living within 10 miles of the plant was eight millirem, and no more than 100 millirem to any single individual. Eight millirem is about equal to a chest X-ray, and 100 millirem is about a third of the average background level of radiation received by U.S. residents in a year."

Three Mile Island has been of interest to human factor engineers as an example of how groups of people react and make decisions under stress. There is general consensus that the accident was exacerbated by incorrect decisions made because the operators were overwhelmed with information, much of it irrelevant, misleading, or incorrect. As a result of the TMI-2 incident, nuclear reactor operator training has been changed. Before TMI, operator training focused on diagnosing the underlying problem; afterwards, operating training focused on reacting to the emergency by going through a standardized checklist to ensure that the core is receiving enough coolant under sufficient pressure.
In addition to the improved operating training, improvements in quality assurance, engineering, operational surveillance and emergency planning have been instituted. Improvements in control room habitability, "sight lines" to instruments, ambiguous indications and even the placement of "trouble" tags (some tags were covering important instrument indications during the accident) have been improved. Improved surveillance of critical systems, structures and components required for cooling the plant and mitigating the escape of radionuclides during an emergency were also implemented. In addition, each nuclear site must have an approved emergency plan which directs the evacuation of the public within a 10 mile Emergency Planning Zone (EPZ) to facilitate rapid notification and evacuation. This plan is rehearsed with federal and local authorities on a periodic basis to ensure that all groups work together quickly and efficiently.
There was also the psychological effect on the nation. Before the accident approximately seventy percent of the general public approved of nuclear power. After this accident, support for nuclear power across the country fell to about fifty percent, where it has remained. The 1979 TMI accident did not, however, initiate the demise of the U.S. nuclear power industry. As a result of post-oil-shock analysis and conclusions of overcapacity, 40 planned nuclear power plants had already been cancelled between 1973 and 1979. No US nuclear power plant had been authorized to begin construction since the year prior to TMI. Nonetheless, TMI added a clearly strong impact on this demise: Of 129 plants approved at the time of TMI just 53 of those not already operating were ever completed. Federal requirements became more stringent, local opposition became more strident, and construction times were vastly lengthened. Note that the two shortest nuclear power plant construction projects were in this same volatile period, River Bend and St. Lucie-2.
The TMI cleanup started in August 1979 and officially ended in December 1993 at a cost of around US$975 million. From 1985 to 1990 almost 100 tonnes of radioactive fuel were removed from the site. However, the contaminated cooling water that leaked into the containment building had seeped into the building's concrete, from which the radioactivity was basically impossible to remove. TMI-2 had been online only three months, but now had a ruined reactor vessel and the containment building was unsafe to walk in - it has been permanently closed. (TMI-1 was restarted in 1985 after overcoming a number of technical, legal, and regulatory hurdles.) Many similar Babcock and Wilcox reactors on order were cancelled - in total, 51 American nuclear reactors were cancelled from 1980 to 1984.
In the end, a few simple water level gauges on the reactor vessel (standard equipment on General Electric, Westinghouse and Combustion Engineering reactors) would have prevented the accident. The reliance on a single indicator, the level in the pressurizer (which was fooled by the turbulence caused by the open valve) essentially caused the meltdown.
|